BASAL MOTOR NUCLEI |
They represent large nuclear masses located deep at the base of cerebrum and in midbrain.
The rules for understanding the concept of basal motor nuclei are:
they extend from the base of cerebrum through the diencephalon to the midbrain
they modulate the somatomotor activity by numerous feed-back circuits connecting them with:
each other (between them)
cerebellum
cerebral motor cortex
Lesions in these nuclei or their pathways result in motor clinical signs as:
muscular rigidity
involuntary movements
Before these nuclei were well known and understood, they were totally called basal ganglia and they were classified as it follows:
Basal Ganglia |
Philogenetical areas represented by different components of Basal Ganglia |
||
Corpus striatum |
Caudate nucleus |
Striatum (Neostriatum) |
|
|
Lentiform nucleus |
Putamen |
||
|
Globus pallidus |
Pallidum (Paleostriatum) |
||
|
Amygdala |
(Archistriatum) |
||
|
Claustrum | |||
Today, all neuroanatomists include the amygdala into limbic system, but the function of claustrum remains unknown. The nuclear masses concerned with the control of the skeleta1 muscular activity were called basal motor nuclei and they include different cerebral, diencephalic and midbrain components as it follows:
|
Basal Motor Nuclei |
|
|
Corpus striatum (Belongs to cerebrum) |
Caudate - Putamen (Striatum) |
|
Globus pallidus (Pallidum) |
|
|
Thalamic nuclei (Belong to diencephalon) |
Ventral anterior nucleus |
|
Ventral lateral nucleus |
|
|
Centrum Medianum |
|
|
Subthalamus (Belongs to diencephalon) |
Subthalamic nucleus (Corpus of Luys) |
|
Zona incerta |
|
|
Midbrain nuclei (Belong to midbrain) |
Substantia nigra |
|
Red nucleus |
|
|
Reticular formation of midbrain |
|
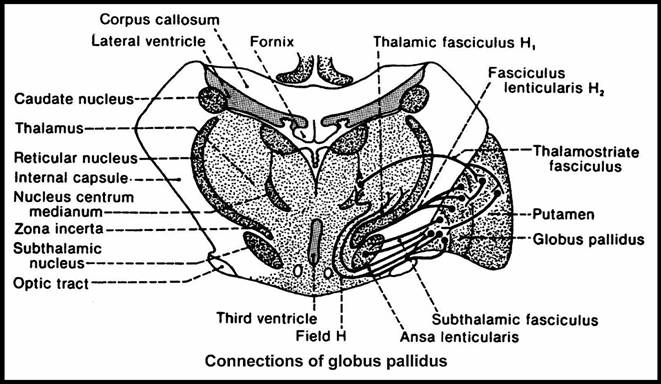
Myelinated axons around basal nuclei form the next formations:
field H of Forel is a bundle of axons which arise from the capsule of fibers around red nucleus and extend dorsomedial;
field H1 of Forel (thalamic fasciculus) conveys 3 major pathways to the thalamus:
pallidothalamic tract
dentatothalamic tract
medial lemniscus
field H2 of Forel (lenticular fasciculus) conveys fibres from globus pallidus to thalamus;
lenticular ansa - it also conveys fibers from globus pallidus to thalamus but it loops under the internal capsule instead to penetrate the internal capsule like lenticular fasciculus;
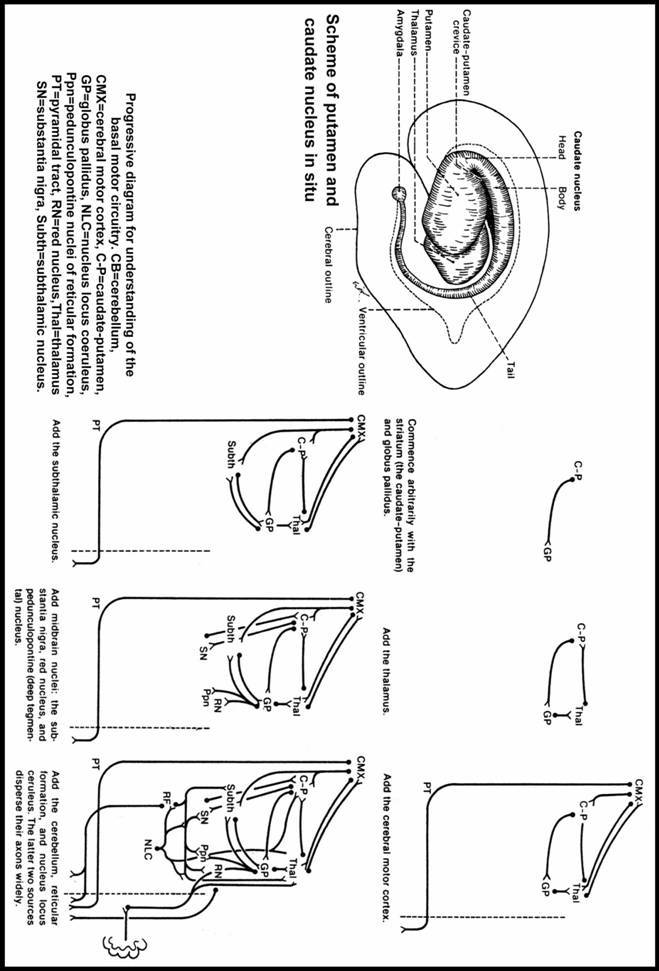
Connections of striatum (caudate-putamen)
afferents
cortico-striatal projections come from pre- and postcentral gyri principally but also from the other areas including the limbic cortex;
thalamo-striatal projections from IL, centrum medianum, and probably VA and VL nuclei;
nigro-striatal afferents arise from pars compacta and pass via internal capsule and field H of Forel;
raphe-striatal afferents.
efferents
striato-pallidal fibres
striato-nigral fibres project through internal capsule to pars reticulata of the substantia nigra;
afferents
striato-pallidal fibres
subthalamo-pallidal fibres via subthalamic fasciculus;
efferents
lenticular ansa
lenticular fasciculus.
subthalamic fasciculus
pallido-tegmental fibres for the pedunculo-pontine nucleus of midbrain reticular formation
as a simplified conclusion we can say that:
pallidum acts as a final common pathway from the basal nuclei to the thalamus and
thalamus projects, in turn, these influences to motor cerebral cortex and from here they are projected down to the lower motor neurons (LMN); this is the most important circuit from clinical point of view
afferents
pallido-subthalamic fibres via subthalamic fasciculus,
cortico-subthalamic fibres from the cerebral motor cortex;
efferents:
subthalamo-pallidal fibres via subthalamic fasciculus
Connections of the red nucleus:
afferents
cortico-rubral fibres come from the ipsilateral precentral gyrus via the internal capsule;
dentato-rubral fibers come from the contralateral dentate nucleus of cerebellum via the contralateral sup. cerebellar peduncle; it decussates just caudal to the red nucleus;
efferents:
rubro-olivary tract descends ipsilaterally in the central tegmental tract;
rubro-spinal tract decussates in the ventral tegmental decussation and enters the lat. funiculus of the spinal cord just ventral to the lat. cortico-spinal tract;
Connections of substantia nigra:
afferents reach mostly the pars reticulata; they are:
striato-nigral fibers which project through the internal capsule
thalamo-nigral fibers are less numerous;
efferents arise mostly from pars compacta; they are:
nigro-striatal fibers traverse globus pallidus after they run superiorly over subthalamic nucleus
nigro-thalamic fibers have the same way like the nigro-striatal ones and project into VL and VA thalamic nuclei;
the concept of extra-pyramidal system includes all the motor pathways of the brain that influence the LMN but do not send their axons directly into the pyramidal tract; it includes:
the circuits of basal motor nuclei,
reticulospinal tract,
rubrospinal tract,
olivospinal tract,
vestibulospinal tract,
tectospinal tract
many authors have argued in favor of abolishing the pyramidal/extrapyramidal concept totally, but clinicians maintain this concept because there are distinctive pyramidal and extrapyramidal clinical syndromes and this concept serves to localise the lesions and to separate different disease entities;
Phylogeny of pyramidal/extrapyramidal system:
in submammals all the movements are extrapyramidal because these animals have no cerebral cortex and no pyramidal tract;
in lower mammals (such as marsupials) the cerebral cortex appears but the pyramidal tract is short and not very useful;
- in lower primates the cerebral cortex and pyramidal tract have an increased importance, but the extrapyramidal system can compensate considerably for the interruption of pyramidal tract
- in humans the movement depends principally on the cerebral cortex and pyramidal system; the next clinico-pathological correlations can be made:
complete unilateral interruption of pyramidal tract paralyses most contralateral voluntary movements, especially of the hand;
complete bilateral interruption of the pyramidal tract paralyses all the voluntary movements of the body caudal to the lesion; the involuntary movements that result from lesions of the basal motor nuclei are also paralysed;
*** as a conclusion we may say that the somatomotor activity is essentially pyramidal in humans; the regulation of this somatomotor activity is made by various afferent pathways that originate in reticular formation, cerebellum, basal motor nuclei and sensory systems and run through the thalamus to the cerebral motor cortex to regulate its activity; the motor cortex, in turn, sends efferences to many of these sources; the lesion of these afferent pathways results in dysmodulation of the cerebral motor cortex which becomes expressed through an intact pyramidal tract by chorea, ataxia and other clinical signs which appear usually on the contralateral side of the lesion;
|
