|
|
|
Sequence and Treatment Procedures |
|
T |
|
he sequence of autotransplantation includes clinical and radiographic examination, diagnosis, treatment planning, surgical procedure, endodon tic treatment, orthodontic treatment, restorative treatment, and maintenance. The criteria for the indications have been discussed in detail in Chapter 4. In this chapter, the sequence and treatment procedures will be discussed. The surgical, endodontic, and restorative aspects of conventional transplantation, intra-alveolar transplantation, and intentional replantation will be covered and illustrated with clinical cases. |
|
Sequence and Procedures of Conventional Transplantation The sequence and procedures of several clinical cases are documented in Fi 545e45f gs 5-1 to 5-16. The reader will note that a variety of treatment approaches have been used. In this chapter, basic and common procedures are discussed by sequence, and particular procedures of each case are explained with graphic illustrations. Examination and diagnosis The examination of potential transplantation patients includes obtaining necessary radiographs and clinical photographs and performing periodontal and soft tissue evaluations and a cariology assessment. Medical and dental specialty consultations also may be needed. Analysis of donor teeth and recipient sites is included as a part of the examination.2-4 Analysis of donor teeth Potential donor teeth must be analyzed for appropriateness of shape and suitability for extraction. If the donor teeth are still developing, the developmental stage of the roots should be 4 or 5 (see Chapter 3). Analysis of recipient sites Mesiodistal and buccolingual widths of the alveolar ridge of the recipient sites and position of the mandibular canal or maxillary sinus should be evaluated. Treatment planning Oral hygiene instruction Unless the caries or periodontal disease causing the nonrestorability of the extracted teeth is controlled, transplanted teeth will follow the same fate. Therefore, oral hygiene instruction, scaling, and root planing must be performed prior to or concurrent with the surgical procedures, and patients should demonstrate an ability to perform oral hygiene.5 Tooth extraction from the recipient site Timing of the tooth extraction from the recipient site should be carefully determined. If the tooth is extracted prior to the date of transplantation, transplantation should be performed 2 weeks to 1 month after the extraction (see Fi 545e45f gs 5-2 to 5-4, 5-7, and 5-8). Indication for same-day tooth extraction with |
|
76 |
|
|
|
|
|
|
|
Sequence and Procedures of Conventional Transplantation |
|
_ij |
|
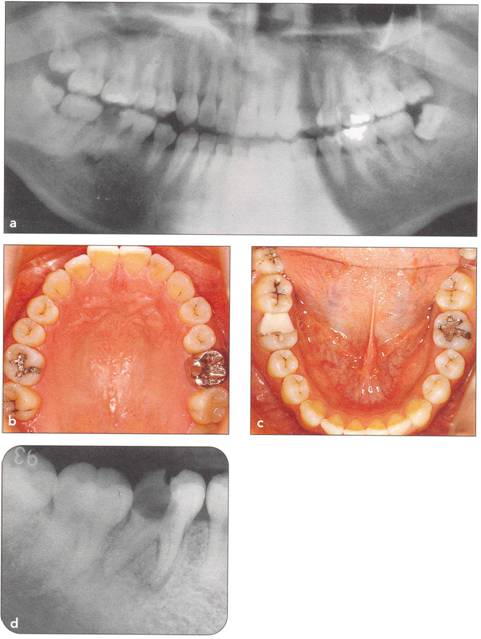
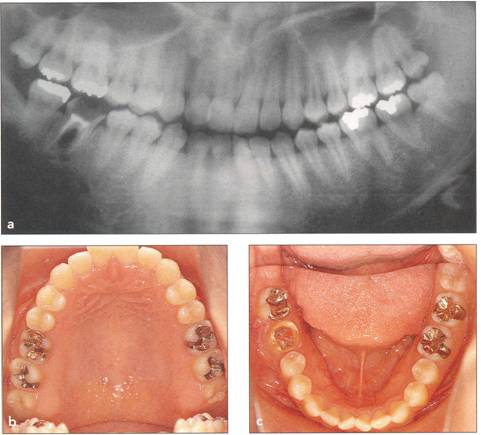
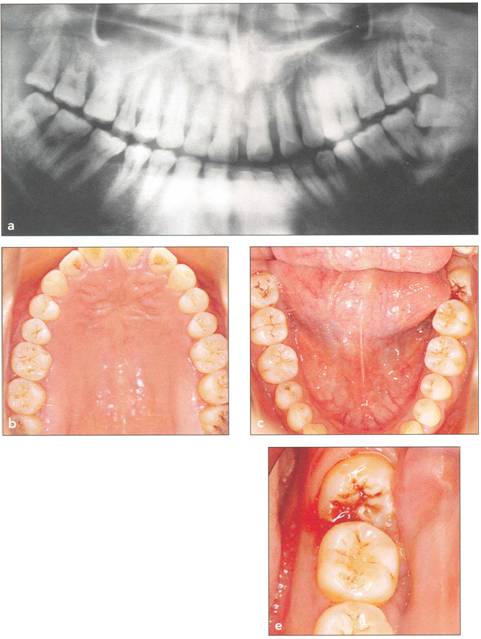
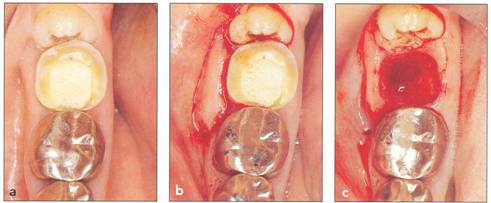
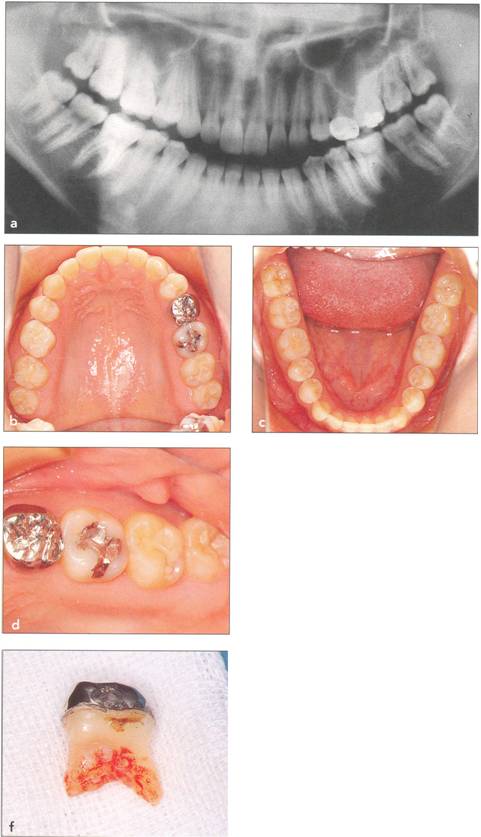
Fi 545e45f g 5-1a Preoperative panoramic view. The patient is a 24-year-old female. Transplantation of the mandibular right third molar to the area of nonrestorable mandibular first molar is planned. |
|
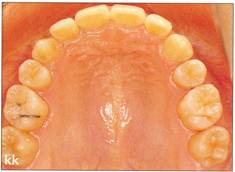
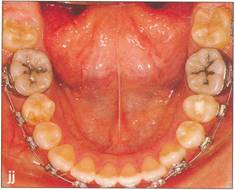
Fi 545e45f gs 5-1b and 5-1c Maxillary and mandibular teeth after initial periodontal treatment of brushing, scaling, and root planing. |
|
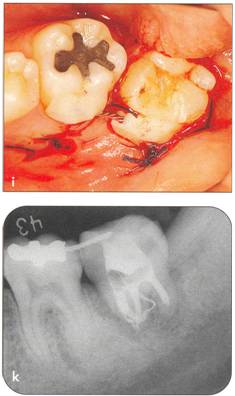
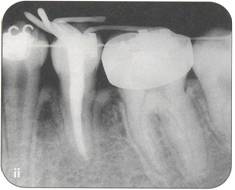
Fi 545e45f g 5-1d Preoperative periapical radiograph. |
|
Fi 545e45f g 5-1e Preoperative view of the donor tooth and the recipient site. |
|
transplantation is determined by the availability of the gingival tissue for pri91ary closure around the transplanted tooth. If the -9iameter of the extraction socket and cervi<;:aJ area of the transplanted tooth are similar, immediate trans plantation is indicatetl (see Fi 545e45f gs 5-1, 5-5, and 5-6), thus sparing the patient the inconvenience of undergoing surgery twice. Another advantage of immediate transplantation is that periodontal ligament tissue in the extraction socket can participate in the healingprocess,- The indication for tooth extraction from the recipient site prior to transplantation is when a discrepancy between the size of the extraction socket and that of the transplanted tooth is expected, resulting in lack of gingival tissue for primary closure. Two weeks after |
|
77 |
|
|
|
|
|
|
|
|
|
|
|
Sequence and Treatment Procedures |
|
II ,c |
|
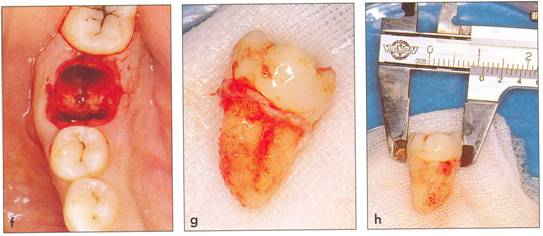
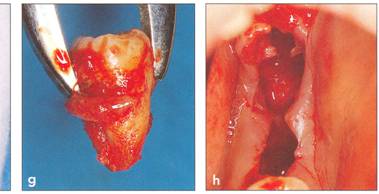
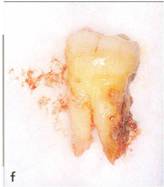
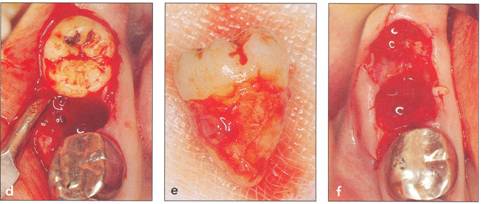
Fi 545e45f g 5-1f After extraction offirst molar from the recipient site. Fi 545e45f g 5-1 g The donor tooth. Note the adequate root form and amount of periodontal ligament on the root. Fi 545e45f g 5-1 h Measurement of the mesiodistal width of the donor tooth. |
|
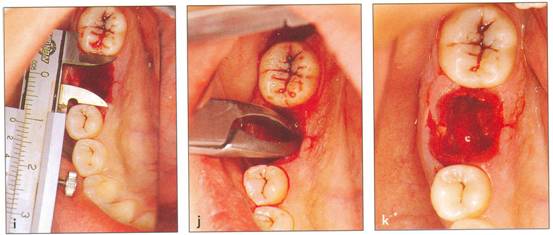
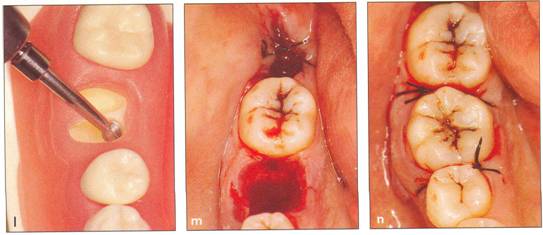
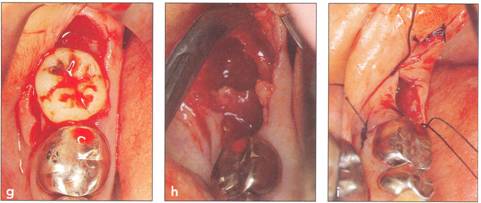
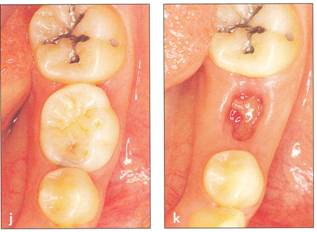
Fi 545e45f g 5-1 i Measurement of the mesiodistal width of the recipient site. If the mesiodistal width of the donor tooth is greater than that of the recipient site, the proximal walls of the adjacent teeth are reduced to fit the donor tooth. Fi 545e45f g 5-1j Preparation of the recipient site. Removal of alveolar septum is done with a minirongeur. Fi 545e45f g 5-1 k After removal of the alveolar septum. |
|
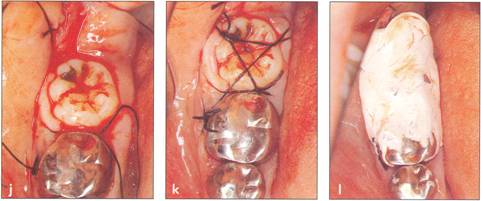
Fi 545e45f g 5-11 Preparation of the recipient site with surgical round burs. Fi 545e45f g 5-1 m Prepared recipient site and extraction site of the donor tooth. Fi 545e45f g 5-1 n After transplantation of the donor tooth and suturing of the flap. |
|
|
|
|
|
|
|
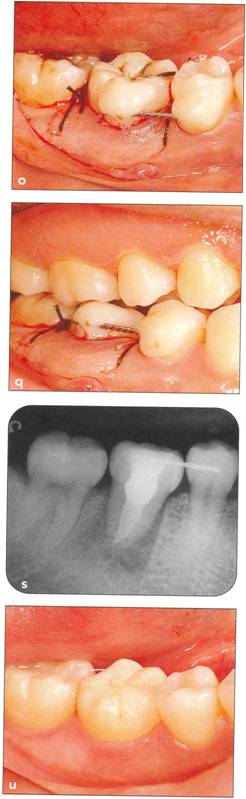
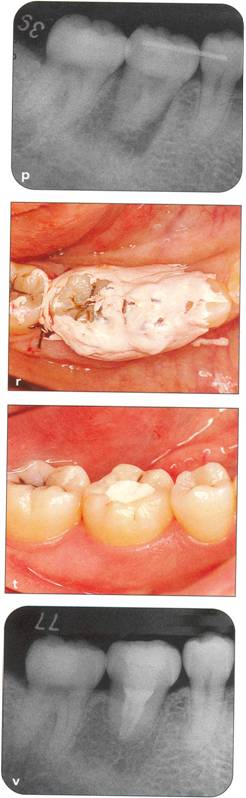
Fi 545e45f g 5-10 Stabilization of the donor tooth. The donor tooth has been splinted to the adjacent tooth with twisted wire and selfcured composite resin after etching and bonding. Fi 545e45f g 5-1 p After transplantation. |
|
Sequence and Procedures of Conventional Transplantation |
|
|
|
II |
|
Fi 545e45f g 5.1q Occlusal relationship after transplantation. The donor tooth is out of occlusion. Fi 545e45f g 5-1r Protection of the wound and prevention of infection by the use of surgical dressing. |
|
Fi 545e45f g 5-15 Three weeks after transplantation. Root canal therapy was started 2 weeks after transplantation. After temporary obturation with calcium hydroxide, the root canal was obturated with gutta percha in 5 weeks. Fi 545e45f g 5-1t Two and one half months after transplantation. |
|
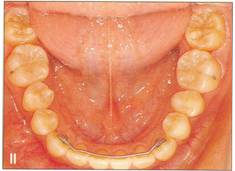
Fi 545e45f g 5-1 u Definitive occlusal restoration of the donor tooth with composite resin. Fi 545e45f g 5-1v One year 3 months after transplantation. Normal periodontal ligament space and lamina dura are observed. |
|
|
|
|
|
|
|
|
|
Sequence and Treatment Procedures |
|
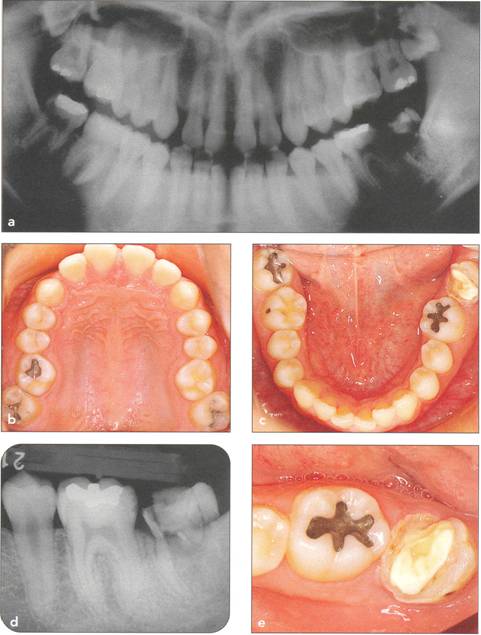
Fi 545e45f g 5-2a Panoramic view on first visit of a nineteen-year-old female patient. The maxillary right third molar will be transplanted to the area of the nonrestorable mandibular right first molar. |
|
Fi 545e45f gs 5-2b and 5-2c Preoperative view of the maxillary and mandibular arches. |
|
Fi 545e45f gs 5-2d and 5-2e Preoperative view of the tooth to be extracted. |
|
extraction, the extraction socket will be covered with enough soft tissue to achieve primary closure. Transplantationshould be performed within 2 months after the extraction because extensive bone resorption will occur after that periQd. Therefore, the ideal timing for transplantation is 2 to 4 weeks after extraction considering the possibility of preservation of the periodontal liga - ment as well as j:Jreparability of recipient sites. Thus, if transplantation is a possibility, the timing of tooth extraction from the recipient site should be considered when the treatment plan is made. |
|
80 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fi 545e45f gs 5-2f and 5-29 Preoperative view of the donor tooth. |
|
Fi 545e45f g 5-2h Extracted donor tooth. This tooth seems to be at developmental stage 6. |
|
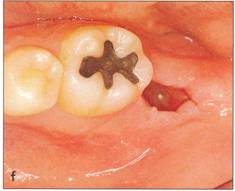
Fi 545e45f g 5-2i The recipient site right before transplant procedure (2 weeks after extraction of the first molar). |
|
f |
|
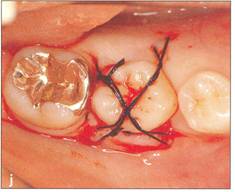
Fi 545e45f g 5-2j After suturing of the gingival flap and fixation of the donor tooth using sutures. |
|
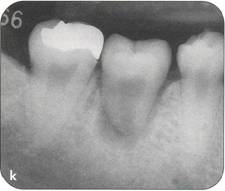
Fi 545e45f g 5-2k After transplantation. |
|
Sequence and Procedures of Conventional Transplantation |
|
|
|
Timing of root canal therapy Root canal therapy should be completed before transplantation or started 2 weeks after transplantation (see Fi 545e45f gs 5-1s and 5-41) with fully developed teeth to prevent inflammatory bone resorption (see Fi 545e45f g 5-6r). |
|
Orthodontic treatment If transplantation is included as part of the orthodontic treatment, position or direction of transplanted teeth can be flexible (see Fi 545e45f g An undesirable size of the recipient site can be improved by orthodontic movement before transplantation. Orthodontic treatment is necessary to correct malpositioned transplanted teeth or problems of osseous (vertical bony) defects around transplanted teeth. |
|
81 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Sequence and Treatment Procedures |
|
Fi 545e45f g 5-21 Two months after transplantation. |
|
Fi 545e45f g 5-2m Two months after transplantation. In a developing tooth, pulpal healing is expected. One must, however, carefully watch for signs of resorption or development of bony lesions indicating pulp necrosis. |
|
Fi 545e45f g 5-2n Eight months after transplantation. Obliteration of the pulp canal from the apex has begun, indicating pulpal vitality. |
|
Fi 545e45f g 5-20 Two years 5 months after trans. plantation. Total obliteration of the pulp canal has occurred, which is a normal outcome. |
|
Fi 545e45f gs 5-2p and 5-2q Two years 5 months after transplantation. The donor tooth is restored with composite resin. |
|
Restorative treatment Unnecessary tooth reduction can be avoided by careful restorative treatment planning (see Fi 545e45f gs 5-1, 5-4, and 5-6). Surgical procedure |
|
The sequence of the surgical procedures is as follows: 1. Setting up instruments 2. Preprocedure administration of antibiotics 3. Disinfection and anesthesia of the surgical sites 4. Extraction of tooth at the recipient site 5. Extraction of the donor tooth 6. Measurement of the donor tooth |
|
82 |
|
|
|
|
|
Sequence and Procedures of Conventional Transplantation |
|
Fi 545e45f g S.3a Panoramic view at the first visit. Maxillary left third molar will be transplanted to the area of nonrestorable mandibular left second molar in a 21-year-old male. |
|
Fi 545e45f gs S.3b and 5-3c Preoperative view. |
|
Fi 545e45f gs S-3d and 5-3e Recipient site before extraction. |
|
7. Evaluation of crown width and try-in ) 8. Preparation of recipient site 9. Try-in and plantation of the donor tooth 10. Trimming and suturing of the flap 11. Fi 545e45f xation and occlusal adjustment of the donor tooth 12. Radiographic evaluation 13. Surgical dressing and home care instructions (including prescription of antibiotics 14. Prophylaxis and removal of pack and suture 15. Removal of splint |
|
83 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Setting up instruments The instruments are shown in Fi 545e45f g 5-17. |
|
Sequence and Treatment Procedures |
|
n |
|
F tl |
|
Preprocedure administration of antibiotics In order to have a desirable antibiotic level in the blood during and after surgery, antibiotics should be taken orally a few hours prior to the procedure. r Penicillin is recommended to achieve rapid increase of antibiotic levels of the blood7;[!etracycline is recommended to maintain high levels of antibiotics in exudate of sulcUS.8-11 |
|
|
|
Fi 545e45f g 5-3f Three weeks after extraction of the second molar. The recipient site is ready for transplantation. Fi 545e45f g 5-3g The donor tooth. |
|
Fi 545e45f g 5-3h The extracted donor tooth. The form of the root and the amount of the periodontal ligament are not ideal. Fi 545e45f g 5-3i Suture of the gingival flap and fixation after transplantation. |
|
Fi 545e45f g 5-3j After transplantation. Fi 545e45f g 5-3k Three months after transplantation. Because healing of the pulp was not achieved, apexification was initiated. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sequence and Procedures of Conventional Transplantation |
|
Fi 545e45f gs 5-3p and 5-3q One year 4 months after transplantation. |
|
Disinfection and anesthesia of surgical site Professional tooth cleaning should be performed before the surgery and the surgery sites should be disinfected. The donor and transplanted teeth and recipient site are anesthetized at the same time. Generally, local anesthesia (including block) is adequate for both extraction and transplantation. |
|
Extraction of tooth at the recipient site If extraction of the tooth at the recipient site is performed the day of transplantation, that extraction should be done prior to extraction of the donor tooth (see Fi 545e45f gs 5-1, 5-5, and 5-6). The periodontal ligament of the extraction socket should not be removed unnecessarily; any endodontic lesion, however, should be curetted as much as possible (see Fi 545e45f gs 5-1j to 5-11). |
|
|
|
|
|
Fi 545e45f g 5-31 Fi 545e45f ve months after transplantation. Fi 545e45f g 5-3m Nine months after transplantation. The calcium hydroxide has been replaced with gutta percha. |
|
Fi 545e45f g 5-3n The donor tooth before restoration with a ceramic crown. Fi 545e45f g 5-30 The ceramic crown. |
|
|
|
|
|
|
|
I_ |
|
Sequence and Treatment Procedures |
|
Fi 545e45f g 5-4a Pretreatment panoramic view. Mandibular left third molar will be transplanted to the area of the non restorable mandibular left second molar in a 39-yearold male. |
|
Fi 545e45f gs 5-4b and 5-4c Preoperative view. |
|
Fi 545e45f gs 5-4d and 5-4e Preoperative view of the recipient site and the donor tooth. |
|
Extraction of the donor tooth If an impacted donor tooth is extracted surgically (see Fi 545e45f g 5-3), alveolar bone over the donor tooth must be removed with a surgical round bur with saline irrigation to avoid damage to the crown or the root. Before elevation of the donor tooth, an incision is made with a blade around the cervical area into the periodontal ligament (see Fi 545e45f g 5-81) to preserve as much periodontal ligament on the root as possible. The extracted donor tooth is immersed in physiologic saline or preservative (see Chapter 3) to prevent drying of the periodontal ligament. The flap of the extraction socket should be closed and sutured to prevent excessive bleeding (see Fi 545e45f g 5-1m). |
|
86 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ill |
|
u |
|
Sequence and Procedures of Conventional Transplantation |
|
f |
|
f |
|
|
|
Fi 545e45f g 5-4f Extracted second molar, which will be discarded. Fi 545e45f g Extracted donor tooth. The amount of periodontalligament is adequate. Transplantation was performed 6 weeks after extraction of the tooth from the recipient site. Fi 545e45f g 5-4h View of the donor site and preparation of the recipient site. |
|
Fi 545e45f g 5-4i After the gingival flap has been sutured and the donor tooth has been splinted. The distal aspect of the donor tooth is closed as tightly as possible. Fi 545e45f g 5-4j After transplantation. Fi 545e45f g 5-4k Two weeks after trans plantation |
|
Fi 545e45f g 5-41 Six weeks after transplantation. The root canals have been cleaned, shaped, and filled with calcium hydroxide. Fi 545e45f g 5-4m Three months after transplantation. The radiograph was taken after removing the splint. Fi 545e45f g 5-4n Seven months after transplantation. |
|
Fi 545e45f g 5-40 Seven months after transplantation. Mesial migration of the donor tooth and regeneration of alveolar bone can be observed. Fi 545e45f g 5-4p One year after transplantation. Fi 545e45f g 5-4q Two years after transplantation. |
|
|
|
|
|
|
|
|
|
Sequence and Treatment Procedures |
|
Fi 545e45f gs 5-4r to 5-4t One year 6 months after transplantation. The donor tooth is restored with composite resin. |
|
Fi 545e45f g 5-4u Three years after transplantation. |
|
Measurement of the donor tooth The size and shape of the donor tooth is determined extraorally to gather information for the preparation of the recipient site. This information is difficult to accurately obtain with preoperative radiographs (see Fi 545e45f gs 5-1h and 580). A caliper or a probe is useful for measuring the mesiodistal or buccolingual width of the crown and the_length 9f the root. The evaluated shape of the root, the length of the root trunk, development of the root (presence of Hertwig's epithelial sheath), and the amount of preserved periodontal ligament should be evaluated and recorded. For these reasons, an extraoral picture of the donor tooth should be taken mesiodistally and buccolingually. |
|
Evaluation of crown width and try-in The distance between the teeth adjacent to the recipient site (if both are present) must be measured and compared to the mesiodistal width of the donor tooth before the final preparation of the recipient site (see Fi 545e45f g 5-1i). If the donor tooth is too wide, a small amount of enamel can be removed from the proximal surfaces of the adjacent teeth and the donor tooth. In total, no more than 2 mm of enamel should be removed when making these adjustments.2 Orthodontic treatment is sometimes indicated to control the space. |
|
88 |
|
|
|
|
|
|
|
|
|
|
|
n t, |
|
Sequence and Procedures of Conventional Transplantation |
|
Fi 545e45f g 5-5a Preoperative view. |
|
Fi 545e45f g 5-5b Incision and reflection of the gingival flap. The incision is made in the gingival sulcus around the tooth at the recipient site and the donor tooth. Vertical incision is made in the distobuccal corner of the first molar. Horizontal incision is made in the buccal corners of the donor tooth and the gingival flap is reflected. |
|
Fi 545e45f g 5-5c After extraction of the second molarfrom the recipient site. |
|
Fi 545e45f g 5-5d Extraction of the donor tooth. |
|
Fi 545e45f g 5.5e The donor tooth. |
|
Fi 545e45f g 5.5f After modification of the recipient site. |
|
Fi 545e45f g 5-59 Try-in of the donor tooth. |
|
Fi 545e45f g 5-5h Releasing incision of the flap. The releasing incision is made in the lingual gingival tissue of the extraction socket of the third molar to achieve better fit of the gingival flap. Fi 545e45f g 5-5i Suture of gingival flap. Before transplantation of the donor tooth, the flap of the horizontal incision and the area of the mesial proximal wall are sutured. One end of each suture is left at 30 mm while the other end of the suture is left uncut. |
|
Fi 545e45f g 5-5j Plantation of the donor tooth. The donor tooth is sealed tightly by the gingival flap because of the flap's elasticity. |
|
Fi 545e45f g 5-5k Fi 545e45f xation of the donor tooth by the sutures. The extra suture is used for fixation of the donor tooth. Extra periosteal suturing of the distolingual area is used for fixation. |
|
Fi 545e45f g 5-51 After application of the surgical dressing to protect the surgical area. |
|
|
|
|
|
n |
|
Sequence and Treatment Procedures |
|
Preparation of recipient site If extraction socket exists. If tooth extraction at the recipient site has been performed within a few weeks before the surgery, an incision is made on the alveolar ridge of the recipient site and in the sulcus of the adjacent teeth with a full-thickness flap to expose 3 to 5 mm of alveolar bone. The incision in the sulcus of the adjacent teeth should be minimal to prevent unnecessary attachment loss. Flap design should be the same even when tooth extraction at the recipient site and transplantation are performed at the same time to allow better direct vision. A vertical incision is made on the distobuccal area of the adjacent tooth to expose more alveolar bone (see Fi 545e45f g 5-5b). After removing any granulation tissue from the extraction socket, the alveolar septum is removed with a rongeur or round bur (see Fi 545e45f g 5-11). If the depth or width of the extraction socket is not sufficient, the lateral or basal wall is recontoured so that the donor tooth can fit passively. |
|
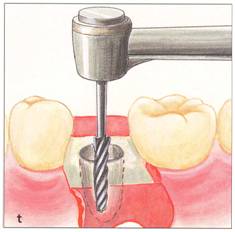
If extraction socket does not exist. When the extraction socket does not exist and the recipient site must be surgically prepared (see Fi 545e45f gs 5-8 and 5-9), the exact position and size of the recipient site and direction of transplantation should be well planned by marking the measured data of the donor tooth on the alveolar bone surface. That is, a reference cut is made corresponding to the size of mesiodistal and buccolingual width of the donor tooth in the cortical bone (Fi 545e45f g 5-8r). Direction and depth are transferred using an implant or trephine bur. It is feasible to use the implant bur when the donor tooth is a premolar, but a surgical round bur should be used when preparing for a molar or making minor adjustments to the recipient site. Preparation of the recipient site should be made with a slow-speed engine (2,000 rpm) while irrigating with saline. |
|
Insufficient buccolingual width of bone. If the mesiodistal recipient space is insufficient for the donor tooth (even after maximum enamel removal), it is necessary to plan orthodontic space generation prior to transplantation. When the bone width is not sufficient buccolingually, either one of the following two methods is indicated: If bone width is far from ideal because of bone resorption, cortical bone is removed using the bur and the bone chisel, then it is placed back around the roots of the transplanted tooth (see Fi 545e45f gs 5-101 and 5100), in the expectation of osteoinduction and bone regeneration (see Fi 545e45f g 3-27). If the insufficiency is minimal, the bone width is increased mechanically using an osteotome or green-stick fracture after the recipient site has been prepared. |
|
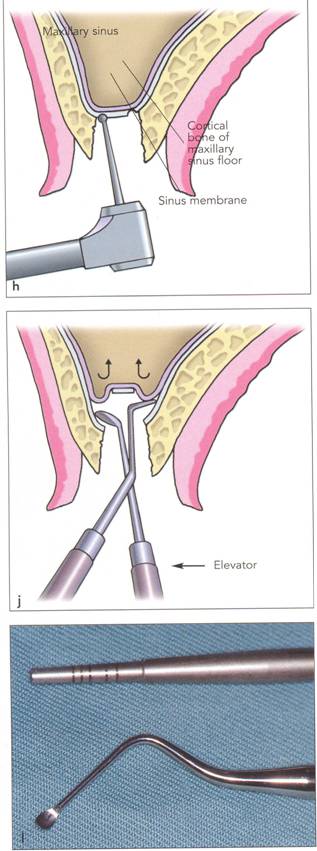
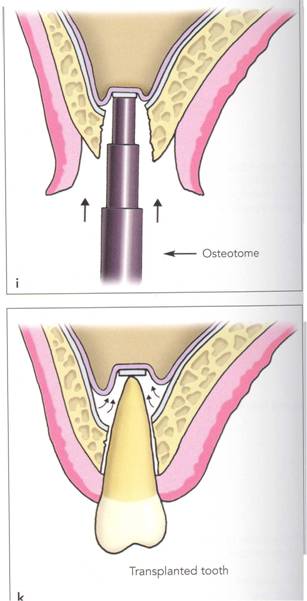
Sinus floor is low; insufficient height of bone. When the sinus floor is low and the height of the bone is shorter than the length of the donor tooth, a sinus lift procedure is indicated12-16 (see Fi 545e45f gs 5-6g to 5-6j) as follows: 1. Recipient site is prepared up to the cortical bone subjacent to the sinus floor. 2. Incision line is made with a round bur on the cortical bone in the area of the sinus floor, with care not to damage the schneiderian membrane (sinus mucosa). 3. Cortical bone plate is slightly lifted into the sinus using an osteotome. 4. Schneiderian membrane is gradually loosened from the sinus floor and gen tly lifted from the space created along the incision line of the cortical bone. |
|
90 |
|
|
|
|
|
|
|
|
|
n |
|
Sequence and Procedures of Conventional Transplantation |
|
Fi 545e45f g 5-6a Preoperative panoramic view. Maxillary left third molar will be transplanted to the area of congenitally missing maxillary left second premolar in a 22-year-old female. |
|
Fi 545e45f gs 5-6b and 5-6c Preoperative occlusal view. |
|
Fi 545e45f g 5-6d Preoperative view of the recipient site and the donor tooth. |
|
Fi 545e45f g 5-6e The recipient site and the donor tooth. Enough height of bone is not available for transplantation because of the level of the sinus floor. |
|
Fi 545e45f g 5-6f Extracted maxillary left deciduous second molar from the recipient site. |
|
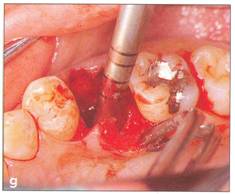
Fi 545e45f g 5-69 Sinus lift. To create space for the donor tooth, part of the bone and mucosa of sinus floor is lifted. (Procedure is explained in detail on the next page.) |
|
|
|
|
|
|
|
|
|
|
|
Fi 545e45f g 5-6i Lifting the bone slightly with an osteotome. |
|
Sequence and Treatment Procedures |
|
|
|
k |
|
Fi 545e45f g 5-6h Pilot drilling on the bone of sinus floor with round bur. |
|
u |
|
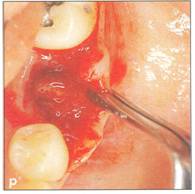
Fi 545e45f g 5-6j Elevation and lifting of the sinus membranewithout damaging it-from the sinus floor with elevators through the space created by lifting the cortical bone. |
|
Fi 545e45f g 5-6k After the procedure. The space between the root, the sinus membrane, and the cortical bone of the sinus floor will be filled with bone. |
|
Fi 545e45f g 5-61 Osteotome and periosteal elevator used for socket lifting. |
|
|
|
|
|
|
|
|
|
u |
|
Sequence and Procedures of Conventional Transplantation |
|
Fi 545e45f g 5-6 (continued) |
|
Fi 545e45f g 5-6m Prepared recipient site. Fi 545e45f g 5-6n The donor tooth. The donor tooth should be extracted prior to preparation of the recipient site and its size and shape should be measured and evaluated. Fi 545e45f g 5-60 Try-in of the donor tooth. Fi 545e45f g 5-6p After satisfactory try-in, the donor tooth is planted in the new site and the soft tissue is sutured tightly around the tooth, which is splinted to the adjacent tooth. Fi 545e45f g 5-6q After transplantation. Fi 545e45f g 5-6r Two months after transplantation. Inflammatory resorption can be observed. Root canal therapy was started immediately. Fi 545e45f g 5-65 Seven months after transplantation. Root resorption has been arrested and the sinus floor elevation has been successful. Fi 545e45f g 5-6t Seven months after transplantation. |
|
|
|
Fi 545e45f gs 5-6u to 5-6w After restoration of the donor tooth. Fi 545e45f g 5-6x One year after transplantation. |
|
|
|
|
|
|
|
|
|
Ii |
|
Sequence and Treatment Procedures |
|
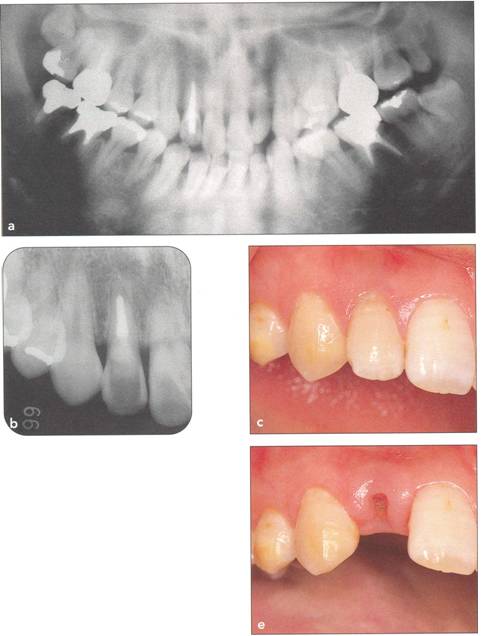
Fi 545e45f g 5-7a Preoperative panoramic view. Maxillary left third molar will be transplanted to the area of the nonrestorable maxillary right lateral incisor in a 34-year-old female. |
|
Fi 545e45f g 5-7b Preoperative view. |
|
Fi 545e45f g 5-7c Recipient site prior to treatment. The patient visited the clinic because of root fracture of the maxillary right lateral incisor in the cervical area. |
|
|
|
Fi 545e45f g 5-7d Removal of fractured fragment. The tooth was extracted because little root length remained. |
|
Fi 545e45f g 5-7e Two weeks after extraction ofthe lateral incisor and just before transplantation. |
|
Try-in and plantation of the donor tooth The donor tooth needs to be tried into the prepared recipient site. Changing the direction of the donor tooth by rotating it 90 degrees helps to find a better fit if the initial direction is not possible. If the depth or length of the prepared recipient site is not adequate, adjustment must be made accordingly by removing bone with round surgical burs. Attention must be paid during the plantation not to damage the periodontal ligament of the donor tooth mechanically by pushing it into the recipient site. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sequence and Procedures of Conventional Transplantation |
|
Fi 545e45f g 5-7f Preoperative view of the donor tooth. |
|
Fi 545e45f g 5-79 The extracted donor tooth. |
|
Fi 545e45f gs 5.7h and 5-7i After transplantation of the donor tooth. |
|
Fi 545e45f g 5.7j Two weeks after transplantation. The root canal has been cleaned and filled with calcium hydroxide. |
|
Fi 545e45f g 5-7k Three months after transplantation. The calcium hydroxide is being replaced with gutta percha. |
|
Trimming and suturing of the flap After try-in of the donor tooth in the recipient site, the fit of the gingival tissues around the donor teeth is checked. The success of transplantation depends on the primary closure of the gingiva around the donor tooth (see Chapter 3). If excess soft tissue is present, the excess is trimmed and the remaining soft tissue is fitted around the donor tooth, making sure that adequate keratinized gingival tissue is available (see Fi 545e45f gs 5-2j, 5-3i, and 5-4i). If there is minimal keratinized tissue at the site, the fitting of the tissue must be done by beveled incision to preserve all keratinized gingival tissue (see Fi 545e45f gs 5-8aa and 5-8bb). |
|
95 |
|
|
|
|
|
|
|
|
|
u |
|
Sequence and Treatment Procedures |
|
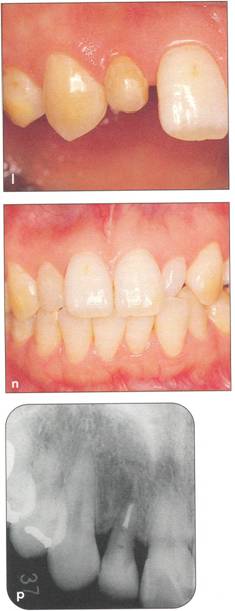
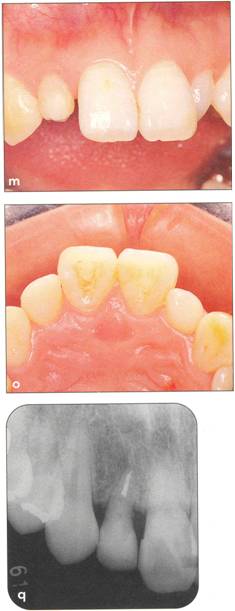
Fi 545e45f g 5-71 Three months after transplanta. tion. Notice the dark appearance of the crown. |
|
Fi 545e45f g 5-7m After bleaching of the transplant. ed tooth. |
|
Fi 545e45f gs 5-7n and 5-70 Composite resin res. toration of the transplanted tooth. |
|
Fi 545e45f g 5-7p Fi 545e45f ve months after transplantation. |
|
Fi 545e45f g 5-7q Three years after transplantation. |
|
When a third molar is transplanted to the area of an adjacent second molar, it may be difficult to obtain a tight fit of the gingival tissue on the distal aspect of the donor tooth. By making a releasing incision, the tissue flap can be brought to a more desirable tight fit to the tooth (see Fi 545e45f g S-Sh). It is easier to suture the vertical incision area or proximal area without the donor tooth in place (the donor tooth can be preserved in physiologic saline) (see Fi 545e45f g S-Si). Plantation of the donor teeth after the suture has been placed is not difficult because of the elasticity of the gingival flap; a better fit actually can be obtained this way. If the suture is to be used for fixation, an extra length of the suture should be for fixation (see Fi 545e45f gs S-Si and S-Sk). 96 |
|
r r |
|
.. |
|
n |
|
Sequence and Procedures of Conventional Transplantation |
|
Fi 545e45f xation and oce/usal adjustment of the donor tooth The type of fixation and its duration depends on various factors. Clinically, stability is important if attachment is to be regained. Although it has been suggested that a long period of fixation after replantation may induce ankyloSiS,17 whether this applies to transplantation is questionable. IS The decision to use wire and bonding resin or a suture for fixation of transplanted teeth must be made based on the needs of each case. |
|
Fi 545e45f xation with wire and resin. Fi 545e45f xation with wire and resin is indicated when it is difficult to stabilize the transplanted tooth because the roots are short or it fits loosely in the recipient site (see Fi 545e45f gs 5-1, 5-3, 5-4, 5-6, 5-7, and 5-10). After<'suturing, the transplanted tooth is fixed to the adjacent anchor tooth (one tooth is sufficient) with acid etched and bonded composite resin and flexible wire on the buccal or lingual side (Fi 545e45f gs 5-17n to 5-17p and 5-18). Fi 545e45f xation with wire and resin also helps retain the surgical dressing, which is the next step, and stabilizes the transplanted tooth during endodontic treatment, which should be started 2 weeks after transplantation. Fi 545e45f xation should be removed in 1 to 2 months. |
|
Fi 545e45f xation with suture. Fi 545e45f xation with a suture is an easy and effective stabilization when the transplanted tooth is stable in the recipient site (see Fi 545e45f gs 5-2, 5-5, 5-8, and 5-9). Gingival tissue is the anchor in this case and a full-thickness flap should not be utilized for this purpose. Periosteum under the gingiva or gingiva around adjacent teeth must be utilized. The suturing of the tissue and the use of sutures for stabilization requires attention to detail and should be carefully planned prior to the surgical procedure (see Fi 545e45f g 5-5). When fixation is performed with suture, occlusal adjustment must be completed before the fixation. The suture should be removed in 5 days. |
|
Occlusal adjustment. The occlusion must be checked to ensure that no occlusal contact is present. If a suture is used for stabilization, the occlusal cOlltacts should be reduced prior to tying the suture; if a wire split is used, the adjustment h done after placing the sprint (see Fi 545e45f g 5-1). The occlusal surface of the donor teeth must be __haped, unless excessive occlusal discrepancy is expected or suture is utilized for fixation. The periodontal ligament must be protected with gauze soaked in physiologic saline during the adjustment. If the opposing tooth is extruded, it must be recontoured prior to the surgical procedure. |
|
Radiographic evaluation Plantation and fixation must be evaluated with radiographs. |
|
Surgical dressing and home care instructions Reattachment of the periodontal ligament from the root of the donor tooth (at the crest of the bone) to the gingival tissues is the first step in healing. Prevention of infection from salivary bacteria is important if reattachment in this area is to be predictable. The transplanted tooth should be protected with surgical dressing for 4 to 6 days after the procedure to enhance healing around the cervical area. Three days of administration of tetracycline after the procedure seems to be effective clinically. After 4 to 6 days the dressing and sutures 97 |
|
Sequence and Treatment Procedures |
|
should be removed and the tooth and surrounding soft tissues cleaned with a cotton swab. The patient should be instructed to brush the area gently. |
|
Removal of the splint The fixation is removed 1 to 2 months after the procedure in cases of fixation with wire and resin. At the time of splint removal, the transplanted tooth should be stable. Root canal treatment (RCT) of the transplanted tooth should be initiated before removing the splint. The following are the recommended procedures after completion of the transplant surgery: RCT, orthodontic treatment, and definitive restoration. |
|
Root canal treatment in transplanted teeth Root canal treatment is necessary in the fully developed donor tooth because healing of the pulp cannot be expected after apical closure (see Fi 545e45f gs 5-1s, 5-41, 5-7j, 5-7k, 5-lOr, and 5-lOs). In the case of an impacted donor tooth, RCT is performed 2 weeks after the transplantation. After preparing the root canals, an interim dressing of calcium hydroxide is placed in the canals. About 2 months later, the calcium hydroxide is replaced with gutta percha and sealer.19 The reason RCT is started 2 weeks after the transplantation is that earlier RCT may affect the attachment around the transplanted tooth and obturation material may damage the periodontal ligament. The advantage of using calcium hydroxide before final obturation is twofold: (1) if the tooth is not fully formed, the calcium hydroxide will promote apical closure and (2) the calcium hydroxide is an excellent antiseptic that will keep the root canal system free from bacterial contamination during the important attachment phase of healing (see Fi 545e45f gs 5-1s, 5-41, and 5-8hh). Root canal treatment performed extra orally at the time of transplantation is both time- and cost-effective. However, there is the risk of damage to the periodontalligament during the procedure, so extraoral RCT is not recommended unless the periodontal ligament can be kept intact during the procedure, which is very uncertain.21 Healing of the pulp is expected with transplanted developing teeth (see Fi 545e45f gs 5-2 and 5-9). Closure of the apex and positive response to electric pulp tests are expected. The roots should continue to develop (see Fi 545e45f gs 5-9k to 5-90). The pulp should be monitered for healing with transplanted teeth at developmental stage 6. Root canal treatment should be started immediately if inflammatory root resorption is suspected (see Fi 545e45f gs 5-60 and 5-8gg), or if irreversible pulpitis is diagnosed. Once closure of the apex with hard tissue after apexification (see Fi 545e45f g 3-37) is confirmed, obturation with sealer and gutta percha is performed (see Fi 545e45f gs 5-3m and 5-8ii). |
|
Natural movement of transplanted teeth After removal of the splint, the transplanted tooth should be allowed to naturally settle into its new position; however, it is advisable to continually check for and adjust any developing occlusal interference. This will ensure that the periodontal ligament attachment and the bony repair proceed properly. During the natural movement and settling of the transplanted tooth, the whole arch will align functionally, providing normal proximal contacts in most instances. |
|
98 |
|
|
|
._ |
|
|
|
|
|
Sequence and Procedures of Conventional Transplantation |
|
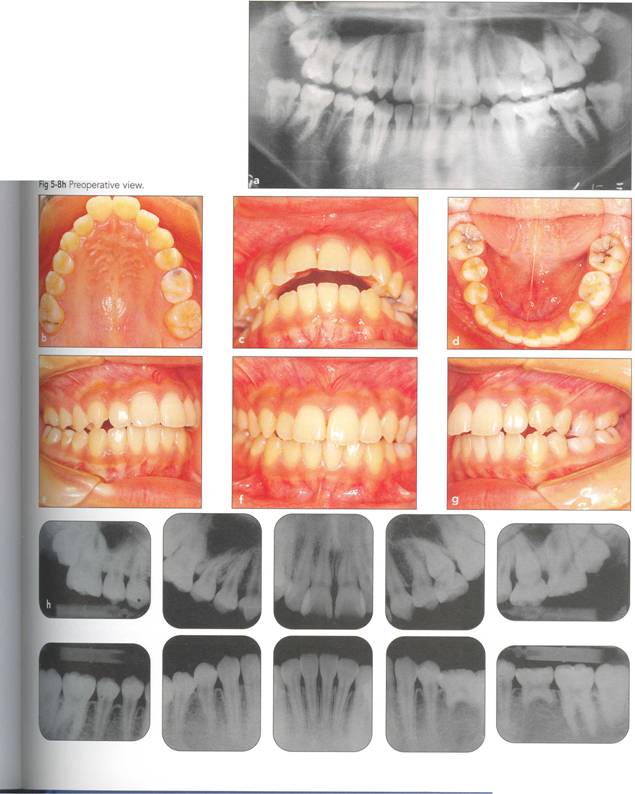
Fi 545e45f g 5-8 Transplantation of an extracted tooth (for orthodontic reasons) to the area of a con genitaJIYrnissingrnandibular premolar. |
|
Fi 545e45f g S.8a Preoperative panoramic view. The maxillary left first premolar will be extracted for orthodontic reasons and transplanted to the area of mandibular left second premolar in a 15year-old female. Fi 545e45f gs S-8b to 5-89 Preoperative intraoral view. Fi 545e45f g S-8h Preoperative view. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
U I,'i |
|
Sequence and Treatment Procedures |
|
|
|
|
|
Fi 545e45f g 5-8i Radiographic evaluation of the donor tooth. Several angulations should be used to determine the likely fit of the donor tooth into the recipient site. If the first premolar is double-rooted, consider using the second premolar as a donor tooth. |
|
Fi 545e45f g 5-8j Preoperative view of the recipient site. |
|
Fi 545e45f g 5-8k Two weeks after extraction of deciduous second molar. |
|
Fi 545e45f g 5-81 Initial incision from the sulcus into periodontal ligament around the donor tooth prior to extraction. |
|
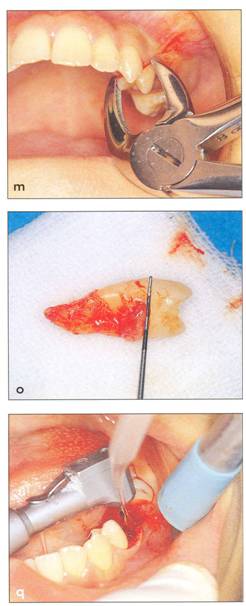
Fi 545e45f g 5-8m Extraction of the donor tooth using diamond-coated extraction forceps for better grip of the tooth crown. |
|
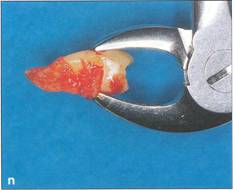
Fi 545e45f g 5-8n Extracted donor tooth. A part of the periodontal ligament was lost. |
|
Fi 545e45f g 5-80 Measurement of the donor tooth. After measurement, the donor tooth is preserved in physiologic saline. |
|
Fi 545e45f g 5-8p Reflection of the gingival flap at the recipient site. A minimal amount of gingival sulcus incision is made on both ofthe adjacent teeth so that attachment loss of these healthy teeth will be minimal. |
|
Fi 545e45f g 5-8q Preparation of the recipient site prior to transplantation. |
|
|
|
|
|
|
|
|
|
|
|
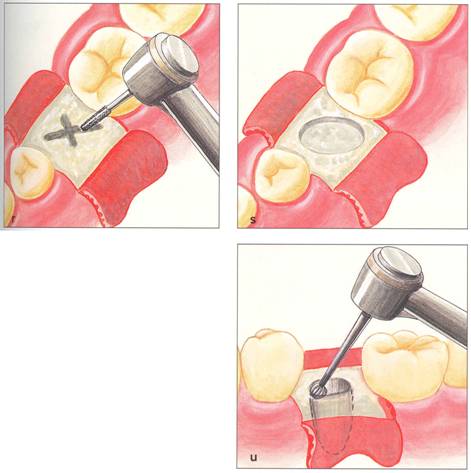
Fi 545e45f gs S-8r to 5-8u The sequence of preparation of the recipient site in an area without a prior extraction socket. Fi 545e45f g 5-8r Use of a bur to mark the size of the socket to be prepared. Fi 545e45f g 5-8s After removal of the cortical plate from the crest of the bone. Fi 545e45f g 5-8t Preparation of the recipient site. The recipient site is prepared slightly larger than the root of the donor tooth; surgical or implant burs can be used for this purpose, running at about rpm. Fi 545e45f g 5-8u Try-in of donor tooth. If the donor tooth is too large, it should be carefully removed and the new socket should be further enlarged. Fi 545e45f g 5-8v Burs for socket preparation. |
|
Sequence and Procedures of Conventional Transplantation |
|
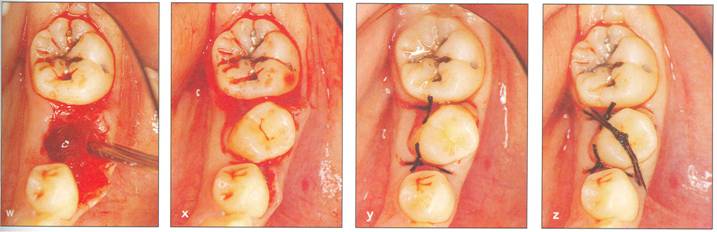
Fi 545e45f g 5-8w The recipient site after the surgical preparation. Fi 545e45f g 5-8x Plantation of the donor tooth. Fi 545e45f g 5-8y Suture placed on the distal and the mesial gingival flap. Fi 545e45f g 5-8z Fi 545e45f xation with a suture. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sequence and Treatment Procedures |
|
|
|
II |
|
II |
|
|
|
Fi 545e45f g 5-8aa An oblique incision made in the buccal gingival tissue to obtain tight closure of proximal gingival tissue. Fi 545e45f g 5-8bb Suture of the area. Tight fit between the gingival flap and the donor tooth can be obtained, thus preserving the keratinized gingiva. |
|
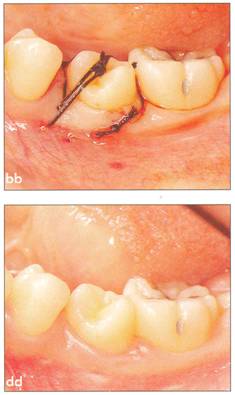
Fi 545e45f g 5-8cc After transplantation. Fi 545e45f g 5-8dd One week after transplantation. |
|
Fi 545e45f g 5-8ee Six weeks after transplantation. Fi 545e45f g 5-8ff Clinical view 6 weeks after trans plantation |
|
Fi 545e45f g 5-8gg Three months after transplantation. Inflammatory root resorption is ob. served on the distal aspect of the donor tooth. Root canal therapy was started immediately. Fi 545e45f g 5-8hh One month after temporary obturation with calcium hydroxide. Arrest of root resorption was confirmed and orthodontic treatment was started. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fi 545e45f g 5-8ii Two years after transplantation. The root canal is being filled with gutta percha, which is replacing the calcium hydroxide initially placed in the canal. |
|
Fi 545e45f g 5-8jj Completion of orthodontic movement. |
|
Fi 545e45f gs 5-8kk to Fi 545e45f g 5-8nn Two years 6 months after transplantation. |
|
Fi 545e45f g 5-800 Two years 6 months after transplantation. Normal appearance of periodontal ligament and lamina dura is observed. |
|
Fi 545e45f g 5.8pp Fi 545e45f ve years after transplantation. |
|
Sequence and Procedures of Conventional Transplantation |
|
|
|